Overview
Pain in the heel of a child's foot, typically brought on by some form of injury or trauma, is sometimes Sever's Disease. The disease often mimics Achilles tendonitis, an inflammation of the tendon attached to the back of the heel. A tight Achilles tendon may contribute to Sever's Disease by pulling excessively on the growth plate of the heel bone. This condition is most common in younger children and is frequently seen in the active soccer, football or baseball player. Sport shoes with cleats are also known to aggravate the condition. Treatment includes calf muscle stretching exercises, heel cushions in the shoes, and/or anti-inflammatory medications. Consult your physician before taking any medications.
Causes
Apart from age, other factors that may contribute to developing Sever?s disease include physical activity, any form of exercise that is weight bearing through the legs or stresses the soft tissue can exacerbate the pain of the disease. External factors, for example, running on hard surfaces or wearing inappropriate shoes during sport. Overuse injury, very active children may repeatedly but subtly injure the bones, muscles and tendons of their feet and ankles. In time, the accumulated injuries cause symptoms.
Symptoms
Pain in the bottom surface and at the back of the heel. Extreme pain when the child places their heel on the ground. The pain is aggravated when running or jumping on hard surfaces. The pain is reduced when the child walks or runs on their toes.
Diagnosis
A doctor or other health professional such as a physiotherapist can diagnose Sever?s disease by asking the young person to describe their symptoms and by conducting a physical examination. In some instances, an x-ray may be necessary to rule out other causes of heel pain, such as heel fractures. Sever?s disease does not show on an x-ray because the damage is in the cartilage.
Non Surgical Treatment
A doctor, sports therapist or physiotherapist can apply a plaster cast or boot if the child is in severe pain. This may be worn for a few days or even weeks and should give relief of pain for a while. Carry out a full biomechanical assessment. This may help to determine if any foot biomechanics issues are contributing to the condition. Orthotics or insoles can be prescribed to help correct over pronation or other biomechanics issues. Prescribe anti-inflammatory medication such as ibuprofen to reduce pain and inflammation. This will not be prescribed if asthma the child has asthma. In persistent cases X-rays may be taken but this is not usual. A doctor, sports therapist or physiotherapist will NOT give a steroid injection or operate as these are not suitable treatment options. The condition will usually settle within 6 months, although it can persist for longer.
Recovery
Sever?s disease is self-recovering, meaning that it will go away on its own when the foot is used less or when the bone is through growing. The condition is not expected to create any long-term disability, and expected to subside in 2-8 weeks. Some orthopedic surgeons will put the affected foot in a cast to immobilize it. However, while the disease does subside quickly, it can recur, for example at the s It is more common in boys, although occurs in girls as well. The average age of symptom onset is 9-11.
Pain in the heel of a child's foot, typically brought on by some form of injury or trauma, is sometimes Sever's Disease. The disease often mimics Achilles tendonitis, an inflammation of the tendon attached to the back of the heel. A tight Achilles tendon may contribute to Sever's Disease by pulling excessively on the growth plate of the heel bone. This condition is most common in younger children and is frequently seen in the active soccer, football or baseball player. Sport shoes with cleats are also known to aggravate the condition. Treatment includes calf muscle stretching exercises, heel cushions in the shoes, and/or anti-inflammatory medications. Consult your physician before taking any medications.
Causes
Apart from age, other factors that may contribute to developing Sever?s disease include physical activity, any form of exercise that is weight bearing through the legs or stresses the soft tissue can exacerbate the pain of the disease. External factors, for example, running on hard surfaces or wearing inappropriate shoes during sport. Overuse injury, very active children may repeatedly but subtly injure the bones, muscles and tendons of their feet and ankles. In time, the accumulated injuries cause symptoms.
Symptoms
Pain in the bottom surface and at the back of the heel. Extreme pain when the child places their heel on the ground. The pain is aggravated when running or jumping on hard surfaces. The pain is reduced when the child walks or runs on their toes.
Diagnosis
A doctor or other health professional such as a physiotherapist can diagnose Sever?s disease by asking the young person to describe their symptoms and by conducting a physical examination. In some instances, an x-ray may be necessary to rule out other causes of heel pain, such as heel fractures. Sever?s disease does not show on an x-ray because the damage is in the cartilage.
Non Surgical Treatment
A doctor, sports therapist or physiotherapist can apply a plaster cast or boot if the child is in severe pain. This may be worn for a few days or even weeks and should give relief of pain for a while. Carry out a full biomechanical assessment. This may help to determine if any foot biomechanics issues are contributing to the condition. Orthotics or insoles can be prescribed to help correct over pronation or other biomechanics issues. Prescribe anti-inflammatory medication such as ibuprofen to reduce pain and inflammation. This will not be prescribed if asthma the child has asthma. In persistent cases X-rays may be taken but this is not usual. A doctor, sports therapist or physiotherapist will NOT give a steroid injection or operate as these are not suitable treatment options. The condition will usually settle within 6 months, although it can persist for longer.
Recovery
Sever?s disease is self-recovering, meaning that it will go away on its own when the foot is used less or when the bone is through growing. The condition is not expected to create any long-term disability, and expected to subside in 2-8 weeks. Some orthopedic surgeons will put the affected foot in a cast to immobilize it. However, while the disease does subside quickly, it can recur, for example at the s It is more common in boys, although occurs in girls as well. The average age of symptom onset is 9-11.
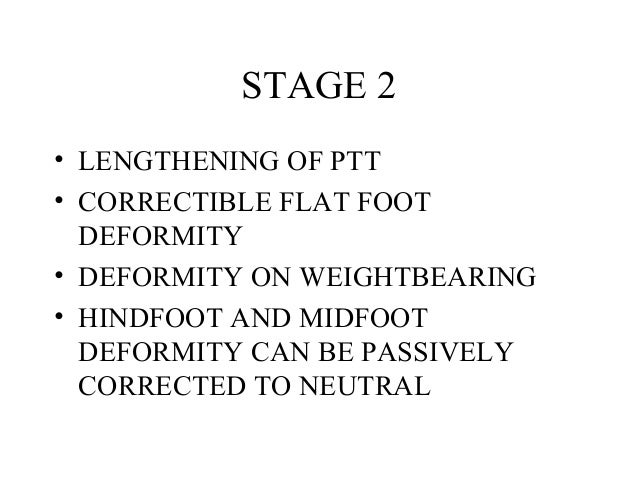 Causes As the name suggests, adult-acquired flatfoot occurs once musculoskeletal maturity is reached, and it can present for a number of reasons, though one stands out among the others. While fractures, dislocations, tendon lacerations, and other such traumatic events do contribute to adult-acquired flatfoot as a significant lower extremity disorder, as mentioned above, damage to the posterior tibial tendon is most often at the heart of adult-acquired flatfoot. One study further elaborates on the matter by concluding that ?60% of patients [presenting with posterior tibial tendon damage and adult-acquired flatfoot] were obese or had diabetes mellitus, hypertension, previous surgery or trauma to the medial foot, or treatment with steroids?. Symptoms Patients will usually describe their initial symptoms as "ankle pain", as the PT Tendon becomes painful around the inside of the ankle joint. The pain will become more intense as the foot flattens out, due to the continued stretching and tearing of the PT Tendon. As the arches continue to fall, and pronation increases, the heel bone (Calcaneus) tilts into a position where it pinches against the ankle bone (Fibula), causing pain on both the inside and outside of the ankle. As the foot spends increased time in a flattened, or deformed position, Arthritis can begin to affect the joints of the foot, causing additional pain. Diagnosis In the early stages of dysfunction of the posterior tibial tendon, most of the discomfort is located medially along the course of the tendon and the patient reports fatigue and aching on the plantar-medial aspect of the foot and ankle. Swelling is common if the dysfunction is associated with tenosynovitis. As dysfunction of the tendon progresses, maximum pain occurs laterally in the sinus tarsi because of impingement of the fibula against the calcaneus. With increasing deformity, patients report that the shape of the foot changes and that it becomes increasingly difficult to wear shoes. Many patients no longer report pain in the medial part of the foot and ankle after a complete rupture of the posterior tibial tendon has occurred; instead, the pain is located laterally. If a fixed deformity has not occurred, the patient may report that standing or walking with the hindfoot slightly inverted alleviates the lateral impingement and relieves the pain in the lateral part of the foot. Non surgical Treatment Treating PTTD is almost always easier the earlier you catch it. So, the first step in treatment is to see your doctor as soon as you begin experiencing painful symptoms. However, once your condition has been diagnosed, your podiatrist will likely try to give the upset tendon a bit of a break so it?ll calm down and stop being so painful. This can often be accomplished by immobilizing the foot using tape and padding, braces, or casts, depending on what your podiatrist believes will work best for you, and depending on the severity of your condition. You may also be instructed to reduce inflammation by applying ice to the area (usually 40 minutes on and 20 minutes off, with a thin towel between you and the ice). Or, you might take anti-inflammatory medications like ibuprofen (steroidal anti-inflammatory meds are actually likely to make this problem worse, and are not usually recommended in treating PTTD), or use ultrasound therapy. Once the inflammation has gone down a bit, your podiatrist may recommend using orthotics (prescription shoe inserts) to support your damaged arch. Ankle braces can also be helpful.
Causes As the name suggests, adult-acquired flatfoot occurs once musculoskeletal maturity is reached, and it can present for a number of reasons, though one stands out among the others. While fractures, dislocations, tendon lacerations, and other such traumatic events do contribute to adult-acquired flatfoot as a significant lower extremity disorder, as mentioned above, damage to the posterior tibial tendon is most often at the heart of adult-acquired flatfoot. One study further elaborates on the matter by concluding that ?60% of patients [presenting with posterior tibial tendon damage and adult-acquired flatfoot] were obese or had diabetes mellitus, hypertension, previous surgery or trauma to the medial foot, or treatment with steroids?. Symptoms Patients will usually describe their initial symptoms as "ankle pain", as the PT Tendon becomes painful around the inside of the ankle joint. The pain will become more intense as the foot flattens out, due to the continued stretching and tearing of the PT Tendon. As the arches continue to fall, and pronation increases, the heel bone (Calcaneus) tilts into a position where it pinches against the ankle bone (Fibula), causing pain on both the inside and outside of the ankle. As the foot spends increased time in a flattened, or deformed position, Arthritis can begin to affect the joints of the foot, causing additional pain. Diagnosis In the early stages of dysfunction of the posterior tibial tendon, most of the discomfort is located medially along the course of the tendon and the patient reports fatigue and aching on the plantar-medial aspect of the foot and ankle. Swelling is common if the dysfunction is associated with tenosynovitis. As dysfunction of the tendon progresses, maximum pain occurs laterally in the sinus tarsi because of impingement of the fibula against the calcaneus. With increasing deformity, patients report that the shape of the foot changes and that it becomes increasingly difficult to wear shoes. Many patients no longer report pain in the medial part of the foot and ankle after a complete rupture of the posterior tibial tendon has occurred; instead, the pain is located laterally. If a fixed deformity has not occurred, the patient may report that standing or walking with the hindfoot slightly inverted alleviates the lateral impingement and relieves the pain in the lateral part of the foot. Non surgical Treatment Treating PTTD is almost always easier the earlier you catch it. So, the first step in treatment is to see your doctor as soon as you begin experiencing painful symptoms. However, once your condition has been diagnosed, your podiatrist will likely try to give the upset tendon a bit of a break so it?ll calm down and stop being so painful. This can often be accomplished by immobilizing the foot using tape and padding, braces, or casts, depending on what your podiatrist believes will work best for you, and depending on the severity of your condition. You may also be instructed to reduce inflammation by applying ice to the area (usually 40 minutes on and 20 minutes off, with a thin towel between you and the ice). Or, you might take anti-inflammatory medications like ibuprofen (steroidal anti-inflammatory meds are actually likely to make this problem worse, and are not usually recommended in treating PTTD), or use ultrasound therapy. Once the inflammation has gone down a bit, your podiatrist may recommend using orthotics (prescription shoe inserts) to support your damaged arch. Ankle braces can also be helpful.  Surgical Treatment Although non-surgical treatments can successfully manage the symptoms, they do not correct the underlying problem. It can require a life-long commitment to wearing the brace during periods of increased pain or activity demands. This will lead a majority of patients to choose surgical correction of the deformity, through Reconstructive Surgery. All of the considerations that were extremely important during the evaluation stage become even more important when creating a surgical plan. Generally, a combination of procedures are utilized in the same setting, to allow full correction of the deformity. Many times, this can be performed as a same-day surgery, without need for an overnight hospital stay. However, one or two day hospital admissions can be utilized to help manage the post-operative pain. Although the recovery process can require a significant investment of time, the subsequent decades of improved function and activity level, as well as decreased pain, leads to a substantial return on your investment.
Surgical Treatment Although non-surgical treatments can successfully manage the symptoms, they do not correct the underlying problem. It can require a life-long commitment to wearing the brace during periods of increased pain or activity demands. This will lead a majority of patients to choose surgical correction of the deformity, through Reconstructive Surgery. All of the considerations that were extremely important during the evaluation stage become even more important when creating a surgical plan. Generally, a combination of procedures are utilized in the same setting, to allow full correction of the deformity. Many times, this can be performed as a same-day surgery, without need for an overnight hospital stay. However, one or two day hospital admissions can be utilized to help manage the post-operative pain. Although the recovery process can require a significant investment of time, the subsequent decades of improved function and activity level, as well as decreased pain, leads to a substantial return on your investment.

 The Achilles tendon is the largest and most vulnerable tendon in the body. It joins the gastrocnemius (calf) and the soleus muscles of the lower leg to heel of the foot. The gastrocnemius muscle crosses the knee, the ankle, and the subtalar joints and can create stress and tension in the Achilles tendon . Tendons are strong, but not very flexible so they can only so far before they get inflammed and tear or rupture. Causes Factors that may increase your risk of Achilles tendon rupture include Age. The peak age for Achilles tendon rupture is 30 to 40. Your sex. Achilles tendon rupture is up to five times more likely to occur in men than in women. Playing recreational sports. Achilles tendon injuries occur more often in sports that involve running, jumping and sudden starts and stops - such as soccer, basketball and tennis. Steroid injections. Doctors sometimes inject steroids into an ankle joint to reduce pain and inflammation. However, this medication can weaken nearby tendons and has been associated with Achilles tendon ruptures. Certain antibiotics. Fluoroquinolone antibiotics, such as ciprofloxacin (Cipro) or levofloxacin (Levaquin), increase the risk of Achilles tendon rupture. Symptoms Patients often describe a feeling of being kicked or hit with a baseball bat in the back of the heel during athletic activity. They are unable to continue the activity and have an extreme loss of strength with the inability to effectively walk. On physical examination there is often a defect that can be felt in the tendon just above the heel. A diagnosis of an Achilles tendon rupture is commonly made on physical exam. An MRI may be ordered to confirm the suspicion of a tear or to determine the extent of the tear. Diagnosis During the physical exam, your doctor will inspect your lower leg for tenderness and swelling. In many cases, doctors can feel a gap in your tendon if a complete rupture has occurred. The doctor may also ask you to kneel on a chair or lie on your stomach with your feet hanging over the end of the exam table. He or she may then squeeze your calf muscle to see if your foot will automatically flex. If it doesn't, you probably have ruptured your Achilles tendon. If there's a question about the extent of your Achilles tendon injury, whether it's completely or only partially ruptured, your doctor may order a magnetic resonance imaging (MRI) scan. This painless procedure uses radio waves and a strong magnetic field to create a computerized image of the tissues of your body. Non Surgical Treatment To give the best prospects for recovery it is important to treat an Achilles' tendon rupture as soon as possible. If a complete rupture is treated early the gap between the two ends of the tendon will be minimised. This can avoid the need for an operation or tendon graft. There are two forms of treatment available for an Achilles' tendon rupture; conservative treatment and surgery. Conservative treatment will involve the affected leg being placed in a cast and series of braces with the foot pointing down to allow the two ends of the tendon to knit together naturally.
The Achilles tendon is the largest and most vulnerable tendon in the body. It joins the gastrocnemius (calf) and the soleus muscles of the lower leg to heel of the foot. The gastrocnemius muscle crosses the knee, the ankle, and the subtalar joints and can create stress and tension in the Achilles tendon . Tendons are strong, but not very flexible so they can only so far before they get inflammed and tear or rupture. Causes Factors that may increase your risk of Achilles tendon rupture include Age. The peak age for Achilles tendon rupture is 30 to 40. Your sex. Achilles tendon rupture is up to five times more likely to occur in men than in women. Playing recreational sports. Achilles tendon injuries occur more often in sports that involve running, jumping and sudden starts and stops - such as soccer, basketball and tennis. Steroid injections. Doctors sometimes inject steroids into an ankle joint to reduce pain and inflammation. However, this medication can weaken nearby tendons and has been associated with Achilles tendon ruptures. Certain antibiotics. Fluoroquinolone antibiotics, such as ciprofloxacin (Cipro) or levofloxacin (Levaquin), increase the risk of Achilles tendon rupture. Symptoms Patients often describe a feeling of being kicked or hit with a baseball bat in the back of the heel during athletic activity. They are unable to continue the activity and have an extreme loss of strength with the inability to effectively walk. On physical examination there is often a defect that can be felt in the tendon just above the heel. A diagnosis of an Achilles tendon rupture is commonly made on physical exam. An MRI may be ordered to confirm the suspicion of a tear or to determine the extent of the tear. Diagnosis During the physical exam, your doctor will inspect your lower leg for tenderness and swelling. In many cases, doctors can feel a gap in your tendon if a complete rupture has occurred. The doctor may also ask you to kneel on a chair or lie on your stomach with your feet hanging over the end of the exam table. He or she may then squeeze your calf muscle to see if your foot will automatically flex. If it doesn't, you probably have ruptured your Achilles tendon. If there's a question about the extent of your Achilles tendon injury, whether it's completely or only partially ruptured, your doctor may order a magnetic resonance imaging (MRI) scan. This painless procedure uses radio waves and a strong magnetic field to create a computerized image of the tissues of your body. Non Surgical Treatment To give the best prospects for recovery it is important to treat an Achilles' tendon rupture as soon as possible. If a complete rupture is treated early the gap between the two ends of the tendon will be minimised. This can avoid the need for an operation or tendon graft. There are two forms of treatment available for an Achilles' tendon rupture; conservative treatment and surgery. Conservative treatment will involve the affected leg being placed in a cast and series of braces with the foot pointing down to allow the two ends of the tendon to knit together naturally. 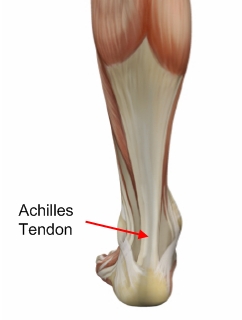 Surgical Treatment Surgery is the most common treatment for this condition. An incision is made in the lower leg and the tendon is sewn back together. A cast, splint, walking boot, or brace is worn for 6-8 weeks. One of the benefits of surgery is that it lowers the risk of re-rupturing the tendon. Surgery may also be a better option if you are athletic. Prevention There are things you can do to help prevent an Achilles tendon injury. You should try the following. Cut down on uphill running. Wear shoes with good support that fit well. Always increase the intensity of your physical activity slowly. Stop exercising if you feel pain or tightness in the back of your calf or heel.
Surgical Treatment Surgery is the most common treatment for this condition. An incision is made in the lower leg and the tendon is sewn back together. A cast, splint, walking boot, or brace is worn for 6-8 weeks. One of the benefits of surgery is that it lowers the risk of re-rupturing the tendon. Surgery may also be a better option if you are athletic. Prevention There are things you can do to help prevent an Achilles tendon injury. You should try the following. Cut down on uphill running. Wear shoes with good support that fit well. Always increase the intensity of your physical activity slowly. Stop exercising if you feel pain or tightness in the back of your calf or heel.
 Achilles tendonitis (tendinitis), is a painful and often debilitating inflammation of the Achilles tendon than can progress into degeneration which we call Achilles Tendinosis. The Achilles tendon is the largest and strongest tendon in the body. It is located in the back of the lower leg, attaches to the heel bone (calcaneus), and connects the calf muscles to the heel bone. In most cases, Achilles tendonopathy's are overuse injuries are more common among athletes and people who train heavily, however it can also occur in people who are less active. Achilles Tendonitis can vary in severity from a mild pain in the tendon during a particular activity to more severe cases when any form of activity that puts strain on this ligament, even standing or walking, can cause pain.
Achilles tendonitis (tendinitis), is a painful and often debilitating inflammation of the Achilles tendon than can progress into degeneration which we call Achilles Tendinosis. The Achilles tendon is the largest and strongest tendon in the body. It is located in the back of the lower leg, attaches to the heel bone (calcaneus), and connects the calf muscles to the heel bone. In most cases, Achilles tendonopathy's are overuse injuries are more common among athletes and people who train heavily, however it can also occur in people who are less active. Achilles Tendonitis can vary in severity from a mild pain in the tendon during a particular activity to more severe cases when any form of activity that puts strain on this ligament, even standing or walking, can cause pain.
 A tendon is a band of tissue that connects a muscle to a bone. The Achilles tendon runs down the back of the lower leg and connects the calf muscle to the heel bone. Also called the heel cord, the Achilles tendon facilitates walking by helping to raise the heel off the ground. The Achilles tendon is at the back of the heel. It can be ruptured by sudden force on the foot or ankle. If your Achilles tendon is ruptured you will be unable to stand on tiptoe, and will have a flat-footed walk. It is important to diagnose and treat this injury as soon as possible, to help promote healing. Treatment involves wearing a plaster cast or brace (orthosis) for several weeks, and possibly having an operation.
A tendon is a band of tissue that connects a muscle to a bone. The Achilles tendon runs down the back of the lower leg and connects the calf muscle to the heel bone. Also called the heel cord, the Achilles tendon facilitates walking by helping to raise the heel off the ground. The Achilles tendon is at the back of the heel. It can be ruptured by sudden force on the foot or ankle. If your Achilles tendon is ruptured you will be unable to stand on tiptoe, and will have a flat-footed walk. It is important to diagnose and treat this injury as soon as possible, to help promote healing. Treatment involves wearing a plaster cast or brace (orthosis) for several weeks, and possibly having an operation.
